
In many communities, the same people who work on preventing the spread of sexually transmitted diseases such as syphilis have been called on to help prevent the spread of COVID-19. Departments are reporting mass interruptions in STD care and prevention services.
- Kaiser Health News, June 4, 2020
Contact tracing is a public health tool that was developed long before the current pandemic. It is an essential element of sexually transmitted disease (STD) prevention and treatment programs that rely on notifying partners of infected persons so that they can be treated with antibiotics in time to stop the chain of transmission. As discussed in the review article "Syphilis: Far From Ancient History" and my accompanying editorial in the July 15 issue of AFP, the national increase in the number of primary and secondary syphilis infections since 2000 has fueled increases in the incidence of congenital syphilis, with 1306 cases diagnosed in 2018.
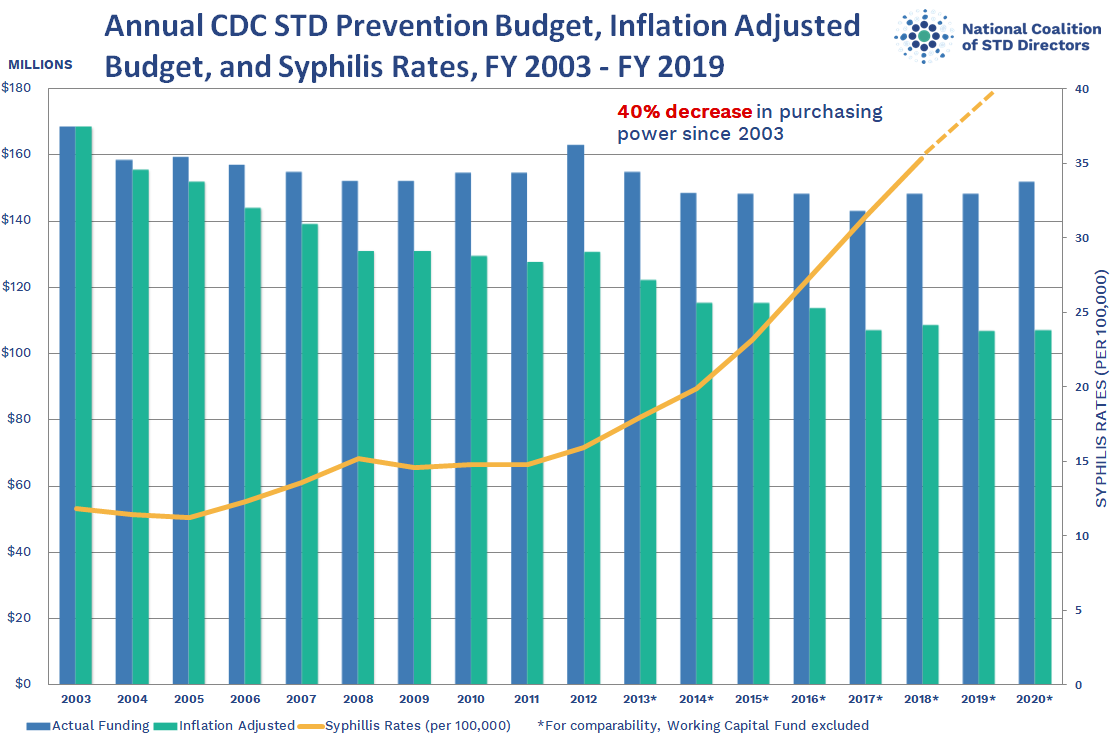
Although the essentially flat (40% decreased in inflation-adjusted dollars) Centers for Disease Control and Prevention (CDC) budget for STD prevention programs since 2003 has likely worsened this problem, a CDC analysis of year 2018 cases identified four types of missed prenatal prevention opportunities that can be addressed by family physicians, obstetricians, and other maternity care providers: 1) lack of timely prenatal care (and consequently no syphilis screening); 2) lack of timely syphilis screening despite timely prenatal care; 3) inadequate maternal syphilis treatment; 4) diagnosing syphilis less than 30 days before delivery. In my editorial, I added that "family physicians can prevent congenital syphilis by following national screening guidelines; taking accurate, detailed sexual histories; providing evidence-based interventions to people who use injection drugs; and advocating to reduce structural barriers to care."
COVID-19 has complicated congenital syphilis prevention by diverting health department personnel who would typically staff STD programs and discouraging expectant mothers from attending in-person prenatal visits due to infection concerns. In a Health Affairs blog post, Dr. Marcus Plescia and Elizabeth Ruebush from the Association of State and Territorial Health Officials affirmed that "there’s nothing non-essential about prenatal care and appropriate testing and treatment for syphilis," and discussed strategies for continuing to provide these critical health care services:

{kind=link}